

With cases of measles on the rise, you may be wondering if you and your family are protected.
We answer ten common questions about measles and the MMR vaccine.
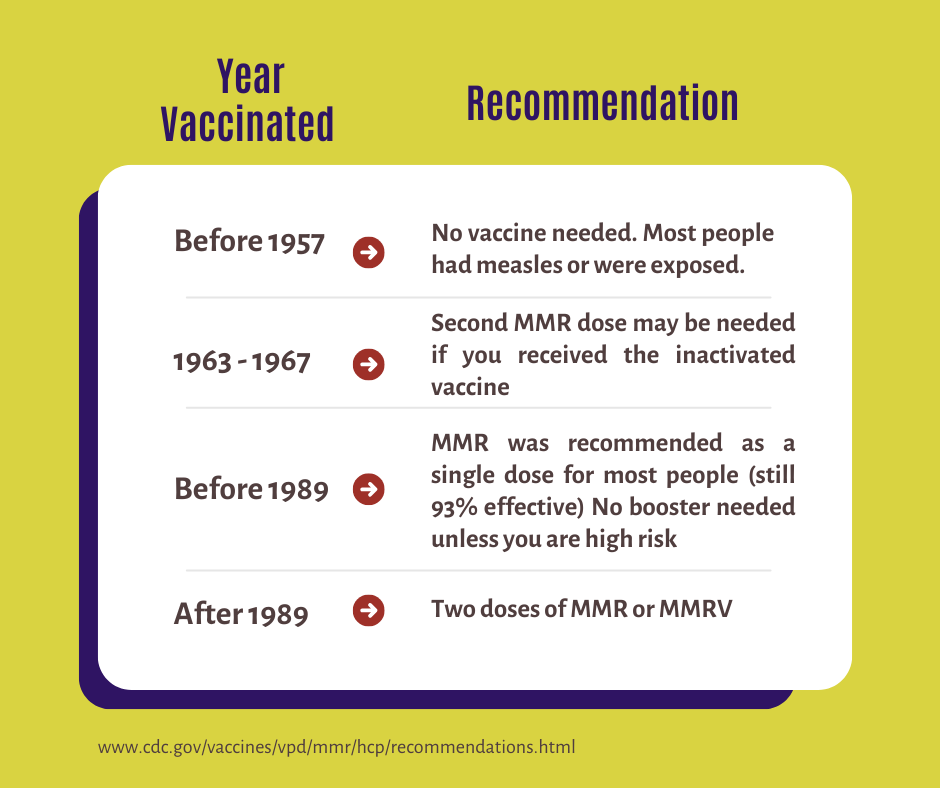
1. How do I know if I’m up to date — do I need a booster?
If you have received two doses of the MMR or MMRV vaccine or were born before 1957, you are considered well protected, and no booster is needed.
You may need a booster if you received the inactivated measles vaccine between 1963 and 1967. Many people received the more effective live vaccine during that time, but if you’re unsure, check with your healthcare provider.
Measles antibodies last a long time. Studies tracking individuals for 17 years found that 91% still had protective antibodies. A single dose of MMR protects for about 25 years, but the vaccine schedule recommends two doses, extending immunity even further. Measles antibodies have an astonishing half-life of over 3,000 years.
2. Do I need to have my antibodies checked?
For most people, probably not.
A titer test checks the level of antibodies in your blood but doesn’t necessarily reflect your level of immunity. Antibodies are just part of your immune system. T cells, B cells, and other immune cells are part of your body’s immune response and are particularly important because once measles enters your body, it doesn’t replicate that fast. So, a negative result on titers does not necessarily mean you are not protected because your B and T memory cells are primed to quickly produce antibodies against the virus the next time it is encountered.
However, insurance may require proof to cover the cost of a booster. Antibody and titer tests should be used only in specific cases, in consultation with your doctor.
3. Is there a reason NOT to get a measles booster shot?
The MMR vaccine is well-studied, safe, and effective, with benefits far outweighing the risks. While some mild side effects can occur, serious side effects are rare.
However, unnecessary boosters could contribute to a vaccine shortage. Approximately 12 million doses are available in the country each year. Vaccines must be available for children since they need at least two doses for initial protection. That population takes priority because children are more vulnerable to serious complications from measles, especially those under 5 years old.
4. Why do we only need two measles shots, but a flu shot yearly?
Measles and the flu are two different viruses that behave and mutate differently. Measles doesn’t mutate nearly as much as influenza does. Today, the measles virus remains virtually unchanged from its 1960s form. The influenza virus mutates every few months. Additionally, the measles virus replicates very slowly and deeply within the body, which gives our bodies time to react. The influenza virus replicates in our nasal passages very rapidly, which makes it difficult for our body to stop it from spreading to others.
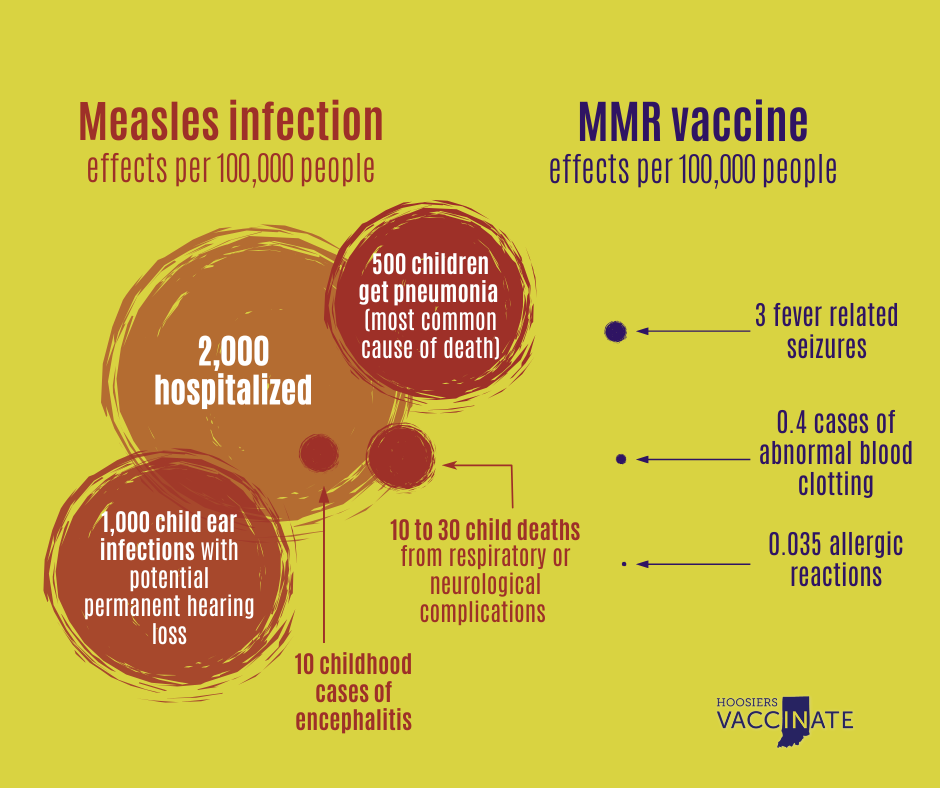
5. Isn’t getting immunity from measles better than vaccine-induced immunity?
Infection-induced immunity may last slightly longer, but it carries a high cost: measles can lead to severe complications, including pneumonia, encephalitis, and death. The purpose of vaccines is to induce immunity without the risks associated with severe infection.
The protection offered by the vaccine is strong and long-lasting. It’s a live virus vaccine, so it’s a minuscule, controlled version of the infection, but with far fewer risks. The risk of complications from the illness far outweighs any risks from the vaccine.
6. Is a baby protected if their mom was fully vaccinated?
While most mothers transfer antibodies to their fetuses, after birth, these antibodies wane quickly and are almost gone by 6-12 months of age. Breastfeeding may provide some protection, but is not a substitute for vaccination. All of this offers some protection until a baby is old enough to receive the first dose of the MMR at 12 months.
6. Can my baby be vaccinated before 12 months?
The vaccine schedule is carefully created by considering several factors, including the waning of maternal antibodies, the maturity of the immune system, and the most common age of infection. However, if you live in an area with an outbreak of measles and have a child between the ages of 6 and 12 months, your pediatrician may offer an early dose of the MMR vaccine. This early dose does not count toward the two-dose series, which will be needed at 12 months.
7. Does my child have to wait until age 4 to get the 2nd dose?
The second MMR dose can be given 28 days after the first, unless it’s the MMRV vaccine, which requires a 3-month gap. This altered schedule is especially useful in outbreak areas. Healthcare providers may recommend a second dose earlier for children aged one to four living in or visiting outbreak areas.
The logic behind waiting until age four to administer the second dose is that most children enter kindergarten at age five, with a higher transmission risk. This timing ensures protection against measles for the roughly 7% of the population that isn’t fully protected from the 1st dose.
8. Can I still get measles even if I’m fully vaccinated?
The MMR vaccine works so well that you are 35 times less likely to get measles than someone without immunity. However, no vaccine is perfect. Three out of 100 fully vaccinated people will get infected; we call these “breakthrough infections.” However, the illness is typically very mild.
Breakthrough infections can be caused by waning immunity or if the person’s immune system didn’t respond to the vaccine in the first place. Roughly 7% of people do not get protection after the first dose, but 95% will be fully protected after a second dose. Only a tiny percentage of people have no response to both doses.
9. Can the vaccine cause measles?
The measles vaccine cannot cause measles because it contains a significantly weakened strain with limited ability to infect and damage cells.
Some have claimed, without evidence, that the measles vaccine caused the outbreak in Texas. The CDC and the Texas Department of State Health Services found that the virus causing the outbreak was a wild measles virus genotype D8, not the weakened vaccine strain, genotype A.
10. Is the vaccine safe?
Yes, the MMR vaccine is well-studied, safe, and highly effective. While vaccines can have side effects, these are typically mild and short-lived, such as fever, rash, or soreness at the injection site.
